Many pathologies can present as a mass in the brain—primary brain cancers, metastases, benign masses, abscesses, parasites, and more—each with its own characteristic locations, appearances and radiological signs. The purpose of this brick isn’t to introduce all of them, but rather, to give the beginner an approach to identify and characterize any cerebral mass.
Intra vs Extra-axial
Cerebral masses can be classified into intra-axial, which refer to masses located within the brain tissue itself, and extra-axial, referring to a mass originating from outside the parenchyma.
Examples of intra-axial masses include gliomas, tumor metastases, cerebral abscesses and more, whereas common extra-axial masses include meningiomas (most common extra-axial tumor in adults!), epidermoids, lipomas, choroid plexus tumors (more common in children), pineal gland and pituitary tumors.
In some cases, distinguishing between intra and extra-axial masses can be as easy as asking yourself “does the mass look like it’s coming from inside the brain tissue or projecting into from an outside source?” Other times, though, it can be harder.
Certain signs exist to help differentiate between extra and intra-axial masses:
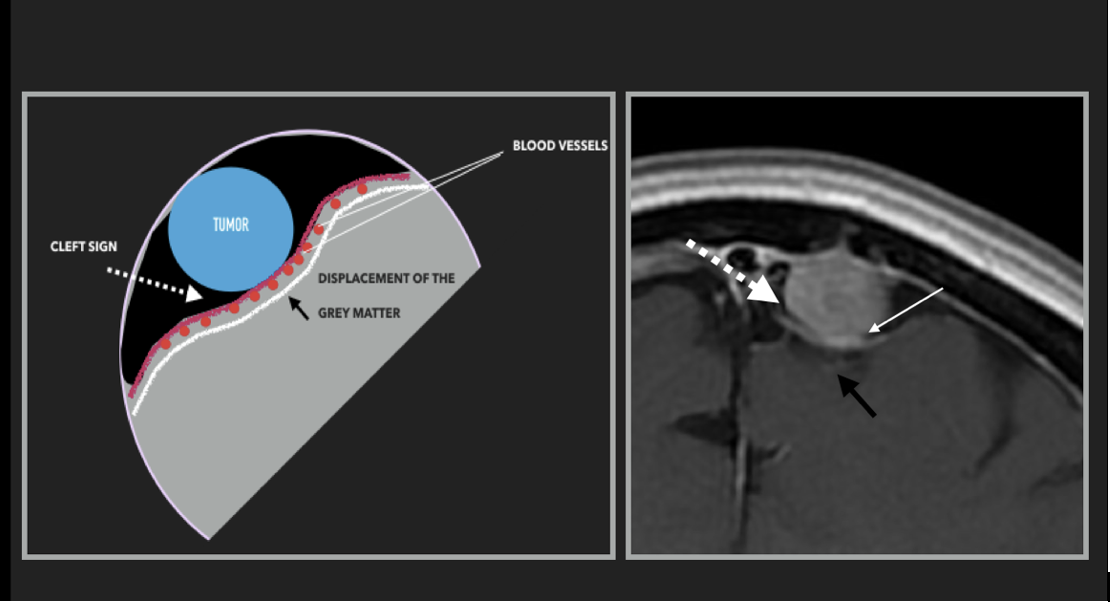
- CSF cleft sign
- When CSF can be seen forming a “cleft” between an extra-axial mass and the brain parenchyma.
- Presence of this sign not only means that the mass is extra-axial, it also helps localize the mass to the subarachnoid space (where CSF is circulating).
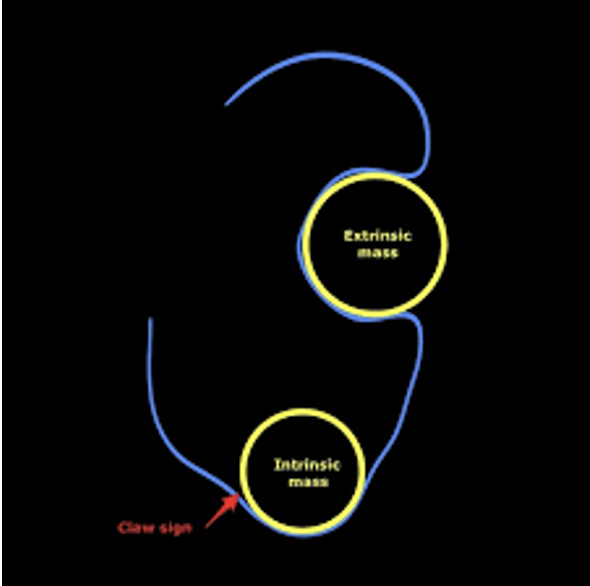
- Claw sign
- This refers to the “sharp” edges formed by the parenchyma around an intra-axial (ie. intrinsic) mass.
- Contrarily, in the case of extra-axial masses, normal parenchyma tends to distort around the mass and would not be seen surrounding the mass on all sides.
- Dural tail
- Represents reactive changes in the dura located near the mass.
- Though most typically seen in meningiomas, a dural tail is NOT specific to them, and can sometimes be seen in other brain masses (including intra-axial ones), though with much less regularity.
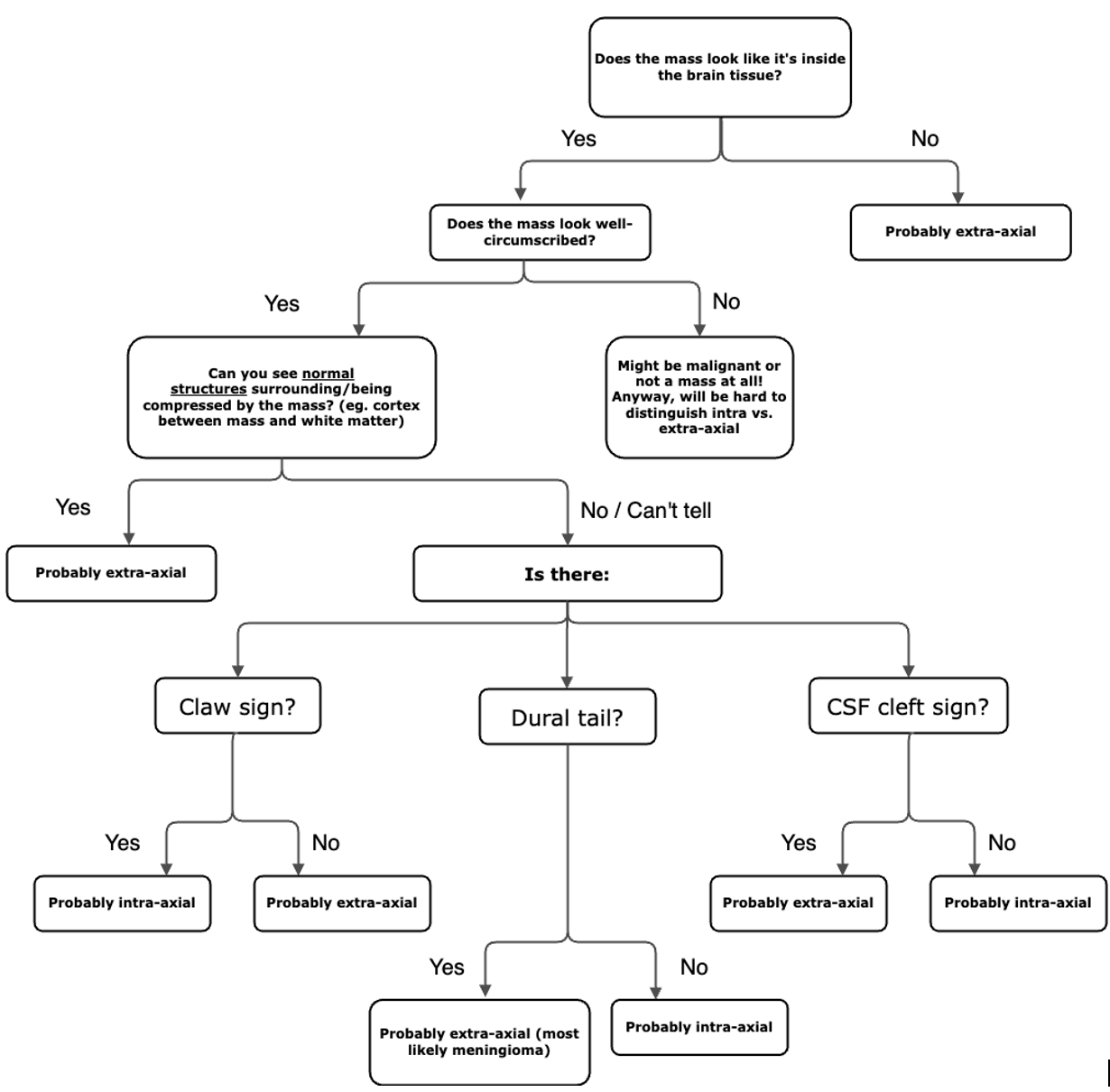
Below is a rudimentary algorithm to differentiate an intra-axial vs extra-axial mass.
Radiological Features
Other than their location of origin, masses can be distinguished based on important radiological features.
Some masses are enhancing with contrast while others are not. The presence of enhancement means that there is disruption of the blood brain barrier (BBB), allowing contrast to enter the brain tissue. However, note that some structures in the brain do not have a BBB and therefore enhance under normal circumstances as well!
List of structures with no BBB:
- Pituitary gland
- Pineal gland
- Choroid plexus
- Extra-axial structures (eg. meninges)
Enhancement can be homogenous or heterogenous and different patterns of enhancement have their own differential diagnoses. For instance, ring enhancing lesions can be suggestive of glioblastoma, metastases or cerebral abscesses. If the enhancing ring is incomplete, then it might suggest an active demyelinating lesion instead.
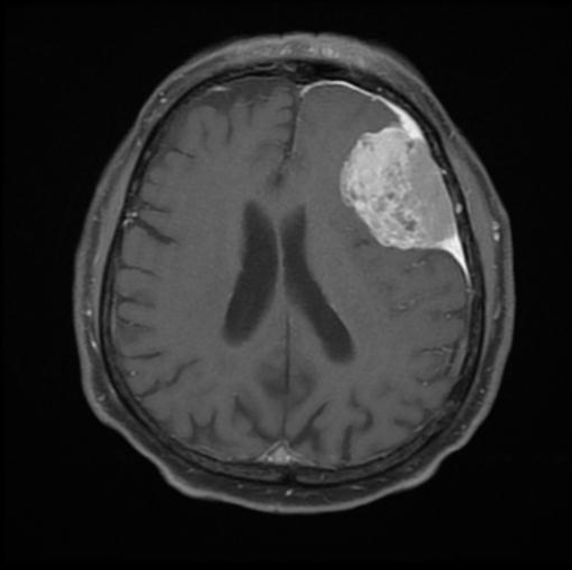
In a similar vein, the border appearance of a mass is also important to note. A well-circumscribed border is more suggestive of a benign tumor or a cerebral abscess (smooth capsule). Meanwhile, if the borders are blurry and you can see the mass encroaching on surrounding tissue (loss of surrounding cortex), then it is more likely a malignancy. The extent and appearance of surrounding edema can also be an important clue.
A rule of thumb is that primary intracranial pathologies will show less impressive surrounding edema than metastases or abscesses (think of something extra-cranial that seeded into the brain), which often present with an edematous area of similar size or even larger than the lesion itself.
Another important feature to note is the number of masses. A solitary mass is more suggestive of a primary intracranial pathology, such as a meningioma or a glioblastoma, whereas multiple masses would make metastases the most important diagnosis to think of.
Finally, when faced with an expansive process, think to look for mass effect. For instance, do the ventricles look symmetric and even? If one or both are larger than normal, there might be an obstructive hydrocephalus caused by the mass. Similarly, is there evidence of cerebral herniation from the mass?
At the very least, expansive processes should cause distortion of local structures, such as the cortex (look for symmetry between the L and R). If you see a lesion with no evidence of even local compression around it, think of other pathologies!
Chronic hematomas, infectious or inflammatory changes (such as demyelinating lesions) can mimic masses so be aware not to tunnel vision on your diagnosis too quick.
Learn more on expansive processes here.